Health and Social Care Committee
Visit to Frankfurt and Lisbon


The Health and Social Care Committee will soon be publishing its report on UK drug policy. This inquiry was informed not only by the evidence we heard from across the UK but also by visits to Lisbon and Frankfurt, where shifts in drug policy have resulted in dramatic reductions in the harm associated with drugs for both those who use them and their communities. We are now sharing what we heard during our visits in advance of publishing our recommendations. Please subscribe to our mailing list in order to be alerted to our full report on October 23rd.
In the week of 15th July 2019, the House of Commons Health and Social Care Committee visited Frankfurt and Lisbon on a joint visit with the Scottish Affairs Committee, as part of our respective drug policy inquiries.

The Health and Social Care Committee's Drug Policy inquiry was launched on 4th February 2019 with a call for written evidence. We have since held 3 oral evidence sessions in Westminster, on the topics of harm reduction, prevention and early intervention, treatment and policing and criminal justice.
Scope of the inquiry


The Committee sought written submissions on the health consequences of illicit drugs policy including on:
Health and harms
What is the extent of health harms resulting from drug use?
Prevention and early intervention
What are the reasons for both the initial and the continued, sustained use of drugs? This refers to the wide spectrum of use, from high-risk use to the normalisation of recreational use.
How effective and evidence-based are strategies for prevention and early intervention in managing and countering the drivers of use? This includes whether a whole-system approach is taken.
Treatment and harm reduction
How effective and evidence-based is treatment provision? This refers to both healthcare services and wider agencies, and the extent to which joined-up care pathways operate.
Is policy is sufficiently geared towards treatment? This includes the extent to which health is prioritised, in the context of the Government's criminal justice-led approach.
Best practice
What would a high-quality, evidence-based response to drugs look like? What responses to drugs internationally stand out as particularly innovative and / or relevant, and what evidence is there of impact in these cases?
Why Frankfurt & Lisbon?


The Frankfurt way
In the 1980s, the open drug scene had congregated in the Taunusanlage Park, near Frankfurt's central station. By the early 1990s, people who used drugs living in the park numbered more than 1,000; drug-related deaths in Frankfurt had rocketed to 147 people in one year, and there were high rates of acquisitive crime.
"We had to recognise that repressive police measures alone are not effective at all”
In 1992, the park was closed and a needle exchange and police van were installed. In 1994, the first (legalised) drug consumption room opened in Germany. In the 1980s the average death of people using drugs was 25; it is now 45. "The Frankfurt Way" was pioneered by the then Christian Democrat Mayor of the city, Petra Roth, working with the Interior and Social Affairs Ministries of the state of Hesse.
Decriminalisation
In 2001, Portugal decriminalised the consumption and possession for personal use of all illicit drugs. The policy was implemented by the Socialist Party, following the declaration of a heroin use epidemic (>1% of the population at the time were reportedly addicted to heroin). By the year 2000, around 50% of incarceration was on drug-related charges. The years following decriminalisation saw a sharp fall in problem drug use, rates of HIV (which fell from 104.2 cases per million in the year 2000 to 4.2 in 2015) and hepatitis, drug-related deaths and drug-related crime.
Frankfurt


We visited Frankfurt’s Police Headquarters, where we met Herr Lars Küthe, Deputy Head of the Narcotics Enforcement Unit, and his colleagues at Frankfurt Police. We heard about the history of Frankfurt’s approach to drug policy, including The Frankfurt Way. We also discussed the cooperation between drug services and police, using the example of drug consumption rooms.
Next, we visited the Hessian Agency for Addiction, where we heard from Managing Director Frau Susanne Schmitt. We discussed Hesse’s approach to drug policy, the different approaches taken in towns and rural areas, and in other Länder (states) across Germany. We also visited the Ministry of Social Affairs, and met Members of the Hessian State Parliament - Herr Moritz Promny, and Frau Kathrin Anders.


Drug Consumption Rooms

We visited three Drug Consumption Rooms (DCR) in Frankfurt: Integrative Drogenhilfe Niddastraße; Eastside; and a Substitutionsambulanz. At Niddastraße we spoke to the Director, Andreas Geremia, about the practicalities of the DCR. Drug users bring their own drugs to consume, and are provided with: health care (with doctors on site at specified times), prevention of infection, first aid in case of overdose, needle and syringe substitution, connection to other services, detoxication, substitution, drug counselling, therapy, medical treatment and rehab.
Lisbon


We visited the Lisbon Commission for the Dissuasion of Addiction (CDT; Comissãos para a Dissuasão da Toxicodependência), where we were hosted by Nuno Capaz, Vice President of Lisbon CDT.
People caught in possession of illicit drugs for personal use are referred to their regional CDT, which is responsible for evaluation, assessment, and where necessary, plan of treatment and follow up. Their main aim is to facilitate a viable healthy lifestyle following a comprehensive approach that tackles both the health and social issues related to drug use. People can also be referred to a CDT by doctors, social workers, family and friends or even do it on a voluntary basis. A person caught by the police in possession of drugs which cannot be considered as solely for personal use will not be referred to the CDT and criminal charges will be opened.


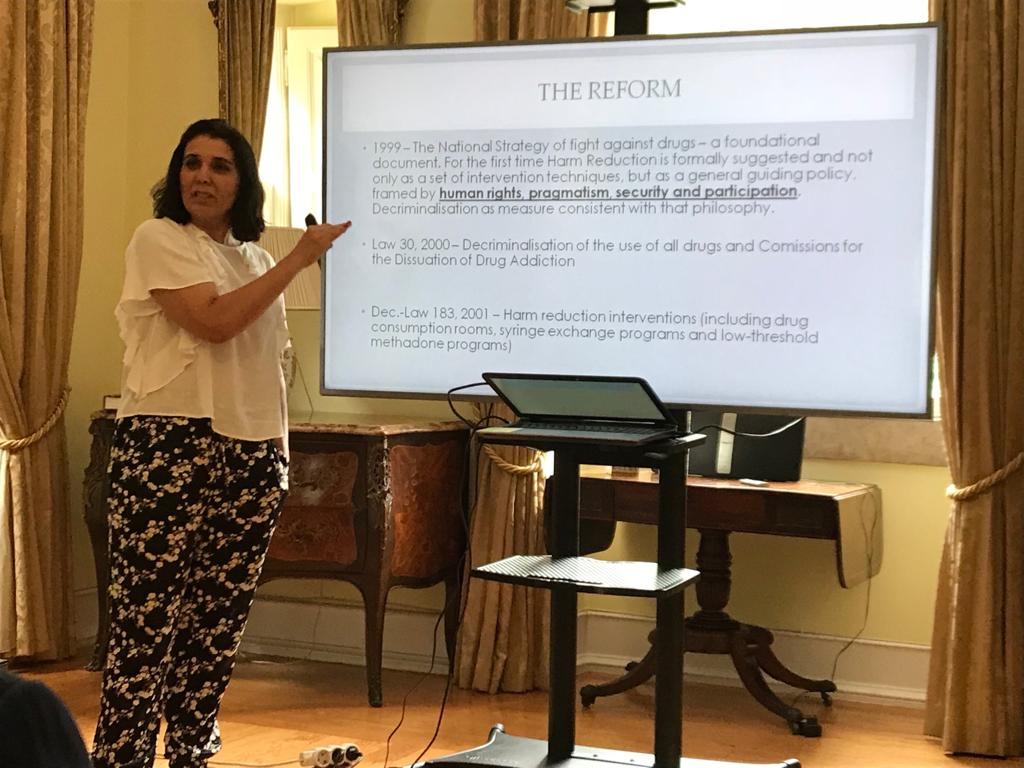
To learn more about the Portuguese reforms and their wider context, we met Marta Pinto, an academic specialising in drug addiction, and Nicola Singleton, an analyst at the European Monitoring Centre for Drugs and Drug Addiction (EMCDDA).


We were introduced to the work of CRESCER, a non-governmental organisation, who work with vulnerable groups at risk of social exclusion. In the afternoon we visited four different projects aimed at helping people who are socially excluded, the vast majority of whom use drugs: É uma rua - (two street teams) É uma casa, a social housing integration project and Espaço Âncora, a drop-in space. We are particularly grateful to CRESCER for giving us the opportunity to speak with people recovering from, or still struggling with, problem drug use, and to see first hand the difference their services are making; and especial thanks to the individuals themselves who bravely and kindly spoke to us, in some cases inviting us into their homes.


At the end of the day we visited a mobile methadone van provided by Association Ares do Pinhal, at one of its regular sites, and learned first hand about the harm reduction services they provide.
Finally, we had the opportunity to meet two Portuguese politicians - Ricardo Baptiste Leite and Ivan Goncalvez - to learn about how the public and political buy-in to make such dramatic changes was secured, and to hear about the challenges facing politicians working in this area today.


Members outside Crescer
Members outside Crescer
Here are some of our Members' reactions to what we saw in Frankfurt and Lisbon:


What we learned
Reform - in the face of crisis

In Portugal in the 1990s there was an opiate epidemic, with 1% of the population addicted to heroin, and a further 0.7% experimenting. At the time a criminal justice-focused approach predominated. A “public health crisis” was declared at the end of 1990s, and a committee was convened in the year 2000, to which a multidisciplinary group of nurses, social workers, and drug users all contributed (see below). The multidisciplinary nature of this group, which included a well-respected scientist, helped the committee to establish credibility with the public, and we heard that the public acceptance of the reform in a conservative country was largely due to the prevalence of problematic drug use, which was spread across all socio-economic groups – every family would care about or know someone who was addicted to drugs. This, apparently, contributed to a change in the narrative, from punitive to personal – where people started thinking: “I know this person – I want to help them”.
From a punitive approach with 50% of incarcerated people being in prison because of a drug-related crime in the 1990s, we heard about the dramatic transformation in Portugal which now can call the police its biggest defender of the decriminalisation approach.
"The “Just Say No” approach was useless – good for voters, but not for users"
In Frankfurt, the high rates of drug use (particularly visible, ‘open’ drug use), acquisitive crime and death in the 1990s precipitated the recognition – by police, politicians and the public – that a punitive approach was not working. A four-pillar approach was designed – incorporating prevention, crisis and survival, drug free programs, and law enforcement. There was an official commitment, as part of a ‘public health approach,’ that a person with a drug addiction be not taken into the criminal justice system until they have had a medical examination. We heard from the police about the cultural change that took place in thinking about drug addiction not as a crime but as an illness. We also heard about the reforms happening contemporaneously with the European Central Bank stationing its headquarters in the centre of Frankfurt, next to the park which was at the time housing 1000 drug users. The ECB provided funding, without which the reforms might not have been possible. We heard from the police that robberies have more than halved since institution of these changes.

What we learned
A public health approach

We heard in both Frankfurt and Lisbon about the move – culturally, legislatively and practically – from a ‘criminal justice’ to a ‘public health’ approach to drugs use.
In Lisbon we heard that, with the radical reforms in the early 2000s, establishing the health structures to provide a much greater offer of health care for people with problem drug use took time. It took over two years to expand health and care capacity sufficiently in terms of funding, workforce and infrastructure. The approach to drug education also changed - education programmes in schools in Portugal are factual, without moral judgement - risks are presented factually (e.g. 'you might develop problems with your memory') like a medical doctor, and education is delivered by psychologists rather than the police.
In Lisbon, we heard frequently about the important role played by SICAD (Serviço de Intervenção nos Comportamentos Aditivos e nas Dependências; General-Directorate for Intervention on Addictive Behaviours and Dependencies), a central agency with responsibility for all aspects of drug policy which has umbrella structure encompassing 1) campaining, 2) housing, 3) NGOs and 4) treatment. Having one central organisation responsible for bringing everything together, including both for funding and for leadership on drug policy, was seen as particularly helpful.
“Setting up the health system took time - budgets, beds and psychologists all needed to increase.”
What we learned
Harm reduction

The Frankfurt Way has a strong focus on Drug Consumption Rooms (DCR) as a form of harm reduction, whereas Portugal’s approach post 2001 has been to focus on other ways of reducing harm to drug users through treatment and decriminalisation (see below). In Lisbon, we heard about some of the challenges of DCRs, which we were told are useful for people who are homeless but are not generally used by people who already have an inside space in which they can take drugs. In Frankfurt DCRs seemed to be a response to problematic ‘open drug scenes,’ but we did also hear about additional benefits of on-site needle and syringe exchange, medical support and linkage into other services.
We heard about various advantages for the drug users of drug consumption rooms: having a closed area and hygienic conditions away from the street; drug deaths have fallen since their institution; drug users are getting older putting them at more risk of harm in the ‘open scene’; and this approach is part of the treatment of people addicted to drugs as disease-oriented rather than criminally-oriented.
We also heard about the advantages of DCRs for the police: there is more security through less consumption in public; there is a central contact for police matters; there is less of a concentration of drug users in public places – which we heard has been associated with reductions in violence and drug-related crime.
Advantages which were cited for the general public: the number of robberies has fallen; 200,000 consumption processes per year happen in DCRs so that public areas, such as parks, are available again to the general public; there are fewer needles in the park/street because of needle & syringe exchange; and there is less littering of drug paraphernalia.
Problems with DCRs that we heard about in Frankfurt were that three quarters of DCRs are located in areas with flats shops and offices; gentrification has meant that new inhabitants in the areas where DCRs operate are complaining about DCRs’ locations and people using the facilities; public budget cuts are putting a strain on services; and a specific problem is that crack consumption is high in Frankfurt– often this is very quick and simple to use so people buy and consume on the street rather than in DCR. We also saw that drug use is more concentrated (even in the street) in the area of the DCR - when you create a DCR all of this market activity takes place in that area (including prostitution etc).


DCRs were recommended by the Committee in Portugal in 2001 but were not implemented. There has been a mobile consumption room since December in Lisbon, which we visited. We were told that since a big barrier to the opening of a DCR is that people often object to their placement in their residential area, a mobile facility is a helpful workaround.
What we learned
Heroin Assisted Treatment


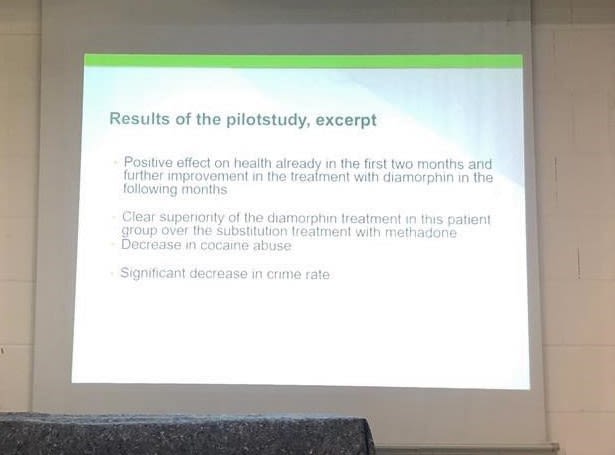
We visited a DCR which provides heroin assisted treatment (HAT) for people with the most problematic addiction to heroin. Diamorphine (heroin) is given to clients, and they inject it themselves. From 2002-07 there was a pilot project in several cities including Frankfurt which found a positive effect on health very early on and clear superiority of the heroin treatment in this group over methadone. There was also a decrease in cocaine use and in the rate of crime. HAT is now provided in 10 cities in Germany. We heard that it is a demanding programme for people accessing heroin, as clients can’t drink alcohol, usually visit the DCR 2 or 3 times a day, and have therapy at the same time, and 90% of patients engaged in HAT in Frankfurt have additional mental health issues. A license for HAT was granted by the Home Office for a service in Cleveland, UK, earlier this year.

What we learned
Decriminalisation

The EMCDDA, whose headquarters we visited in Portugal, produced a video which explains the decriminalisation of drugs.
We heard the successes of the approach in Portugal to decriminalisation of personal possession of drugs in Portugal with reported reductions in harm, crime and heroin use. In implementing the reforms post 2001, the Portuguese government has moved spending from criminal justice to health. There has been a dramatic reduction in drug related deaths since 2001, as well as anecdotal reports of reduced stigma. While drugs are still illegal to supply, people caught in possession now have a full risk assessment carried out by the CDT and are referred on to treatment where necessary, allowing early intervention and strengthening access to treatment. We were also told that generally people are now happier to call for an ambulance if a friend has accidentally overdosed.
We heard that decriminalisation does not have an impact on access - people still cannot buy drugs legally, but if caught it is the person dealing, rather than the person buying drugs who would be arrested.
We heard from the EMCDDA that Portugal's approach is a good model. But the whole package, and not just legislative change, is crucial. Deaths and harms have been successfully reduced; drug use hasn’t disappeared, but concerns about a surge in use or of drugs tourism have not materialised. But we received a very clear message from all quarters that it would be a mistake to look at drugs policy just from a decriminalisation angle and that a comprehensive response is needed – we were told that the results would have been totally different without the holistic model implemented in Portugal post-2001.
“The history of drug policy tells us that it is comprehensive policies, not decriminalisation alone, that reduce harm"
What we learned
Challenges

In Frankfurt, whilst Drug Consumption Rooms had clearly been part of relocating drug users from the city's park, we saw public consumption outside the DCRs we visited (outside of their normal opening hours) and in the streets around them. It was also pointed out by some of our hosts, as mentioned above, that a degree of the pressure to disperse the 'open drug scene' from the central park was due to the location of the European Central Bank, which provided funding - leading to questions about reproducibility of this approach elsewhere.
We also discussed the variation in the offer of harm reduction and treatment in different states in Germany: we heard that Hesse has a much more expansive offer than neighbouring Bavaria, which has a higher rate of drug related deaths. We were told that drug users travel from Bavaria to Hesse (predominantly Frankfurt) to access drug services. This led to questions about the implications of differential drug policy in the different countries of the United Kingdom.
In Lisbon many of the people we met spoke frankly about the challenges that still remain in Portugal, indicating that drugs are an ongoing problem, and that the current situation is still far from perfect. There were various issued raised including:
• More action needed to address drug use in prisons;
• Problems with definition of 'personal use';
• Lack of understanding of the law amongst some law enforcement professionals, with a need for improved training for the new generation of police officers;
• Ongoing under-funding;
• Lack of access to drug treatment and psychological support – while some people we met described rapid, next-day access to treatment, others reported that users could have to wait up to 2-3 months for treatment in some cases;
• Drug users remaining dependent on methadone for extended periods of time, in some cases over 20 years, suggesting a focus on health is not enough – we heard some people arguing that a focus on protecting drug users human rights would be more appropriate, would safeguard people’s dignity, and stop drug users being ‘forgotten’.
What's next for the Drug Policy Inquiry?
Our report, containing recommendations for the Government, will be published shortly.
The Committee is extremely grateful to all those who organised and facilitated the visits to Frankfurt and Lisbon, and to those who contributed their time and expertise.

Detailed information from our inquiry can be found on our website.
If you’re interested in our work, you can find our more on the House of Commons Health and Social Care Committee website. You can also follow our work on Twitter.


The Health and Social Care Committee is a cross-party committee of MPs appointed by the House of Commons to examine the policy, administration and expenditure of the Department of Health and Social Care and its associated bodies.